
The purpose of this blog is to create awareness on some of the effects of combined hormonal contraceptives or CHC’s, especially to those women who struggle with symptoms where non-hormonal/other reasons have been ruled out as the cause of their pain. I am not against the use of “the pill” in any way, especially if it is indicated as the best option for you, as there are multiple reasons for women to be on “the pill”. Always consult with your pelvic floor Physiotherapist or Gynaecologist if you present with these symptoms.
First, let me start by explaining the words “vulvodynia” and “vestibulodynia”. These are symptoms many women struggle with and it is complex as there are multiple causes and reasons for it:
Vulvodynia: pain in the vulva, it is a symptom. Pain usually, but not always, from penetration during intercourse or insertion of tampon, finger, speculum etc. Sensations like burning or irritation in the vulva area are present in patients struggling with vulvodynia.
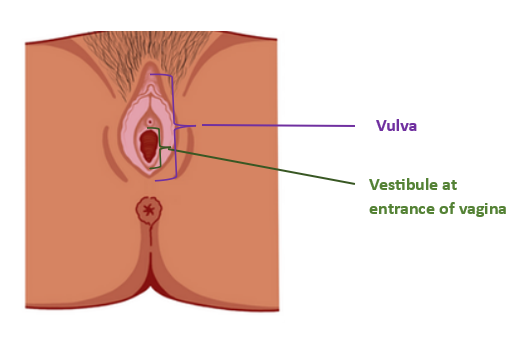
Vestibulodynia: is usually a localized provoked pain in the vestibule which is at the entrance of the vagina. The pain experienced is usually sharp and/or burning but it is localized to the vestibule. The pain is most often brought on during sexual activities where penetration is involved. Both Vulvodynia and Vestibulodynia can lead to Dyspareunia (painful intercourse/pain with intercourse)
Vulvodynia and Vestibulodynia can be caused by co-morbidities (previously existing condition or disease), genetics, hormonal changes or problems, inflammation in the area, musculoskeletal reasons such as weakness or tension, neurologic problems, psychosocial reasons or trauma and structural changes. But in this blog, we will be looking at possible effects on the vulva during CHC use which might lead to vulvodynia or vestibulodynia.
Combined Hormonal Contraceptives’ Mechanism of Action.
What happens to your hormones and cycle pattern while on “the pill”?
*”The pill” suppresses ovulation by inhibiting the pituitary gland from producing and secreting follicle-stimulating hormone (FSH) and luteinizing hormone (LH) (The pituitary gland is at the base of the brain, important for production and secretion of hormones for bodily functions and growth as well as maintaining function of other endocrine/hormone producing glands)
In non CHC using females (what naturally happens when not on “the pill”) FSH: Follicle stimulating hormone, stimulates follicles on the ovary to grow before ovulation, and as these follicles’ size increase, they begin to release estrogen and a low level of progesterone into your blood. FSH also prepares the eggs for ovulation. LH: Luteinizing hormone helps to regulate the length of the menstrual cycle. It triggers ovaries to create steroid hormones in order to start ovulation and the release of an egg, as well as implantation of an egg in the uterus.
*When on “the pill”: There is a decrease or stop of mid-cycle surge of FSH and LH- therefore no ovulation as described above
In non CHC using females (what naturally happens when not on “the pill”): The Corpus Luteum is a collection of cells forming in the ovary during the surge in LH during ovulation. The LH surge usually stimulates the formation of the corpus luteum- most important function is producing progesterone in order to change the uterus into a healthy and proper environment for fetus development
*When on “the pill”: Follicle development, ovulation and corpus luteum formation is therefore inhibited.
*There is then an absence of progesterone production due to no corpus luteum formation. This leads to a stop in the preparation of the endometrium lining for egg implantation, therefore no support for pregnancy – unable to fall pregnant
* OVARIAN estradiol and testosterone secretion is reduced, which leads to no ovulation and might affect sex drive.
* Reduction in serum-free testosterone (FT) – might contribute to a lowered desire for sex, low mood and energy. (Serum free testosterone heightens sex drive and mood in non CHC using females to promote reproduction.)
Can changes to the vulva occur while on “the pill”?
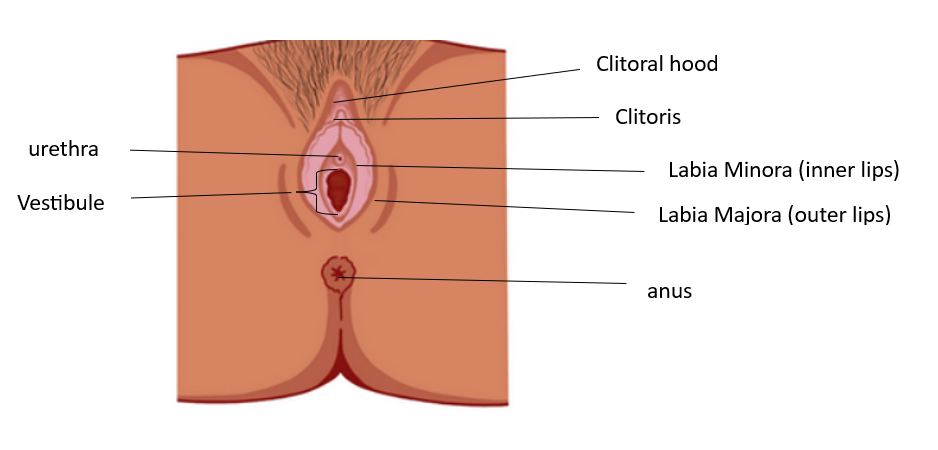
Some studies showed that there could be some changes in the epithelium, smooth muscle and stroma (these are skin, muscle and other soft tissue) when on continuous CHC. These areas depend on estrogen and androgens (serum free testosterone) and are hormonally dependent, but while on “the pill” the levels of these hormones are lower- this might lead to the vulva becoming mildly atrophic (Atrophy means diminished muscle mass or wasting away). CHCs might in some cases lead to some macroscopic and microscopic changes in the vulva. In some cases a mild reduction in the size of the labia minora, clitoris and the diameter of the vestibule have been noticed.
Effect on arousal and Lubrication while on “the Pill”
Some studies have noted a decrease in lubrication due to the use of CHCs. Lubrication fluid during arousal is secreted by the glands in the vestibule of the vulva (Bartholin’s glands, Skene’s glands and other minor vestibular glands). These glands depend on androgens/testosterone for optimal function. There is a likelihood that the decrease in Testosterone (serum free testosterone) due to CHC use might cause dysfunction of these glands – which in turn might cause changes or decrease in arousal and lubrication.
So it is understandable how these changes in hormones, the vulva and lubrication can contribute to pain in the vulva or vestibule and in turn then also have an effect on arousal. There are studies that demonstrated there is a relationship between the use of CHC’s and provoked vestibulodynia. It has been noted that long term use of CHC’s, especially before the age of 17, pose a greater risk for developing provoked vestibulodynia. But let’s not forget that there are certain conditions, like endometriosis, that can benefit from being on “the pill”. (Goldstein AT. Hormonal Causes of Dyspareunia. Female Sexual Pain Disorders: Evaluation and Management. 2020 Aug 20:63-8.)
If Vulvodynia/vestibulodynia is caused by the use of CHC’s (and other causes have been ruled out) then the best treatment would be to stop the use thereof, although it is understandable that this might not always be an easy option for some women. A compounded topical cream preparation that consists of estradiol and testosterone, prescribed by a Gynaecologist or Sexiologist, have been shown to decrease pain symptoms (this is a cream that can be directly applied to the vulva). But the most common treatment combination is topical cream application, pelvic floor physiotherapy and prescribed oral medication treatment.